[Messageboard]
![]()
|
|
Inhaled Insulin: An Overview
John R. White, Jr., PA-C, PharmD, and R. Keith Campbell, MBA, RPh, CDE Introduction: Various methods of insulin administration other than injection have been sought since the discovery of insulin. For the past several years, systems that deliver insulin via the pulmonary route have been developed and evaluated. Based on available data, pulmonary insulin appears to be safe, efficacious, and well accepted by patients. This article describes the technology behind several of these pulmonary administration systems and outlines the most recent data from clinical trials evaluating pulmonary insulin.
History: The first patient to receive a dose of insulin was 14-year-old, 65-lb Leonard Thompson. He received an impure injection of 15 ml, which was described as “a thick brown muck,” on January 11, 1922. His blood glucose fell slightly, and because of the impurities in the extract, he developed an abscess at the site of one of his injections.1 Since then, a plethora of purer forms of insulin and insulins with various time action profiles have been produced, approved, and administered.2 Protamine zinc insulin was introduced in the 1930s. NPH was introduced in the 1940s. The lente series was introduced in the 1950s.2 Advances in chromotography in the 1960s and 1970s led to the production of highly purified insulins. In the 1980s, recombinant DNA technology was used to produce human insulin. Insulin was the first drug ever produced by recombinant technology. More recently, DNA technology has led to the ability to synthesize insulin analogs. To date, more than 300 insulin analogs have been produced.2 While the purity of insulin has increased and the needle size for injections has decreased, thus reducing the discomfort associated with subcutaneous insulin injections, no method of insulin delivery other than injection is currently available. The concept of nasally administered insulin first appeared in 1935.3 Unfortunately, low bioavailability and great variability in absorption found in research done thus far have demonstrated that nasally administered insulin is not particularly practical. Several years ago, interest in the possibility of administering insulin via the pulmonary route surfaced. Since that time, several methods have evolved that may eventually bring this idea to fruition. This article briefly reviews the physiological and pharmacological basis for pulmonary insulin and discusses several of the more salient systems currently being evaluated in the United States.
Rapidly acting pulmonary insulin: Recent technological advances have made it feasible to deliver insulin to the alveolar space. Here, it is rapidly absorbed into the alveolar capillaries and disbursed throughout the systemic circulation. Alveolar epithelium measures ~100 m2 (the size of a tennis court).4 This extremely vascularized surface is very permeable, making inhaled insulin an attractive alternative to injections. The absorptive ability of the alveolar surface stands in contrast to the thick layered mucosoa of the upper airways and the bronchial tree, which are relatively impermeable to peptide drugs. Until quite recently, insulins administered via the pulmonary route in human studies were soluble, rapid-acting formulations. Technology is now available that may allow for the pulmonary administration of longer-acting, as well as rapid-acting, insulin compounds.
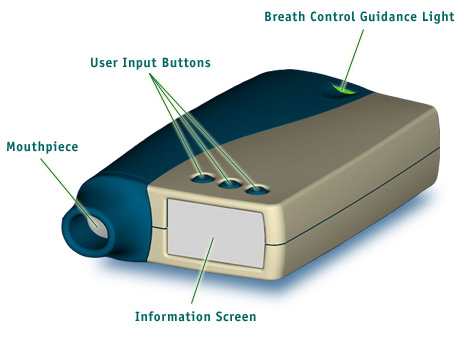
Inhalational Systems: Two of the more well-known and highly publicized inhalation systems are those from Inhaled Therapeutics of San Carlos, Calif., which is working in collaboration with Pfizer and Aventis, and from Aradigm Corporation of Hayward, Calif. These two systems use different technology to deliver insulin via the pulmonary route.
1) The Inhaled Therapeutics
system : Inhaled Therapeutics uses a technology it developed called “PulmoSol powder technology” to create the right-sized particles to reach the deep lung. These particles are highly soluble and quickly dissolve upon reaching the alveoli. They then pass a single cellular layer into the circulation. Powdered aerosolized particles can contain up to 95% pure drug, in contrast to aqueous aerosols, which typically contain only 1 or 2% drug and about 98% water. These powder aerosols carry approximately five times more drug in a single breath than does a metered-dose inhaler system and much more drug than do liquid or nebulizer systems.5 The PulmoSol glass
stabilization system : Insulin from this system will be available in “blister packs” and will remain stable at room temperature for up to 2 years. The device used with the Inhaled Therapeutics system is the size of a mechanical flashlight and is very easy to use.
(Click on the image for a larger view)
Long acting Pulmonary
insulin : Unfortunately, the doses required in this trial were very high. Doses of 9 mg of powder were administered to rats weighing 0.3 kg. This would be roughly equivalent to a 2,100-mg dose for a 70-kg human—a mass probably too large to be inhaled on a regular basis. Inhalational Systems: 1) AIR :
Conclusion : Several viable methods for the pulmonary delivery of insulin are currently in development. Based on available data, pulmonary insulin appears to be effective and safe. While the majority of insulin delivery systems being evaluated use rapid-acting insulin, systems are also being developed that may allow for the administration of long-acting insulins. Ease of administration of pulmonary insulin may lead to better compliance and better glycemic control in the long run.
|
 About
the following article : This article is a
review paper published by the authors mentioned below. We at KEMates have had
nothing to do with editing the paper, except for formatting it (i.e. making the
headings more prominent etc..) and adding the photographs. The following article
has been placed in the public domain i.e. we can publish the article without
permission as long as we credit the original authors with it.
About
the following article : This article is a
review paper published by the authors mentioned below. We at KEMates have had
nothing to do with editing the paper, except for formatting it (i.e. making the
headings more prominent etc..) and adding the photographs. The following article
has been placed in the public domain i.e. we can publish the article without
permission as long as we credit the original authors with it. This device uses a fine-powdered formulation. The particle size used in this system is less
than 5 µm in diameter.4,5 Particles of this size are able to reach the deep
lung with slow, deep inhalation. Larger particles are more likely to become
lodged in the upper airway, while smaller particles will be partially exhaled.5
This device uses a fine-powdered formulation. The particle size used in this system is less
than 5 µm in diameter.4,5 Particles of this size are able to reach the deep
lung with slow, deep inhalation. Larger particles are more likely to become
lodged in the upper airway, while smaller particles will be partially exhaled.5