[Messageboard]
![]()
|
|
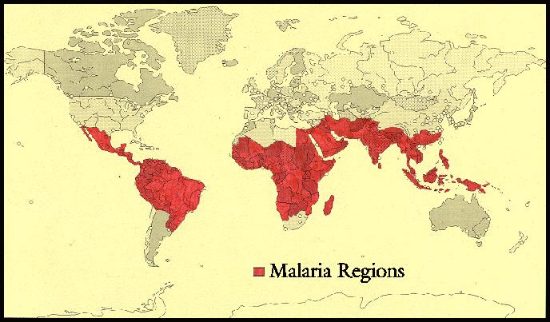
World Distribution of Malaria :
A
Cure for Indifference The
Financial Times,
May 5, 1999 by Michael and
Jeffrey Sachs Nobody knows the exact extent of malaria - which may reach 500m cases a year and 2.7m deaths - but all agree that the toll on human welfare and economic development is profound. Advances in science have now made it possible for us to seek to eliminate the disease. We believe the key to success lies in harnessing the world's biotechnology industry in the struggle. Great strides in vaccine research and in the science of malariology offer realistic hopes that an effective anti-malaria vaccine could be developed within a decade. The sequencing of the malaria genome will soon be complete and a number of promising potential vaccines have already been identified. The critical problem is finding the money for vaccine research, development, and distribution. There is simply not enough money in malaria, as drug companies know. Malaria is a tropical disease, in which a parasite is spread between humans by the bite of an infected mosquito. Since the mosquitoes can transmit the disease only in warm temperatures, the disease is highly concentrated in tropical climates. But people in the tropics are overwhelmingly poor and in no position to pay for vaccines, and so drug companies have little incentive to research them. As a result, malaria vaccine research is carried out mainly in government research institutes, all suffering from underfunding and competing claims on scarce budgets. The Wellcome Trust estimated recently that worldwide malaria research amounted to $84m annually, or perhaps $42 per malaria fatality. This expenditure is tiny relative to that on diseases affecting richer and more temperate areas. For example, research funding for asthma is around $800m annually or $500 per fatality. In short, the 2.4bn people in the tropics that are vulnerable to malaria provoke remarkably little research effort. This problem was recognized a few years ago by leading scientists and policymakers. In an important meeting in Washington in 1995, some of the world's leading scientists in malariology recognised that "a malaria vaccine is feasible", but that a "co-ordinated strategy for vaccine development . . . is essential". We believe that these scientists identified part of the solution, by calling for increased support for public malaria research and a "Malaria Vaccine Development Board" to help mobilise global science. But we think an additional step is needed.
Governments in rich countries are reluctant to commit these funds without a guarantee that a vaccine would be effective. Pharmaceuticals are developed by profit-oriented private companies. It generally costs around $300m to develop, test and bring to market a new medicine. A malaria vaccine may cost several times as much, given the scientific challenges involved. Such development costs are a critical barrier to developing an effective vaccine.Without a sizeable market at the end of the process, no private company will undertake the risky and costly path of vaccine development. That sizeable market is nowhere in view. Not only are the malaria victims themselves very poor, but the existing international agencies that might buy the vaccines on their behalf are themselves strapped for cash.
We propose that public policies should be organised to provide an adequate market at the end of the development process. Leading governments should pledge today that they will help purchase for mass distribution an effective malaria vaccine whenever such a vaccine is successfully developed. They should promise to pay a realistic price that that would cover development as well as production costs. No large bureaucracy would be needed to choose among scientific approaches, or subsidise development efforts - although government support for basic research would continue. Such a programme need not be prohibitively costly. Around 90 per cent of malaria cases, including almost all of the worst variety, are in sub-Saharan Africa. Some $250m annually would be sufficient to purchase vaccine for the 25m children born in Africa each year at $10 for a course of treatment. Even at $40 per child - a large amount for a vaccine widely distributed in developing countries - the cost would be only $1bn to produce a vaccine worth many times that amount. A committee of scientific and health experts could establish criteria for eligible vaccines, and determine procedures for purchasing vaccines once they become available. This initiative would clearly be worth the investment. Foreign aid to Africa now totals around $16bn per year, so that at $10 per child the anti-malaria effort would amount to 1.5 per cent of total aid. Even at $40 per child, the cost would still be only 6 per cent of the aid effort. Furthermore, unlike aid programmes of uncertain effectiveness, the vaccine funds would only be spent when a proven vaccine was developed.
Spending such sums each year would be a very small price to help protect Africa against a disease that kills 2m or more people a year, and that cripples economic development. With the financial backing of the richest countries in the world mobilising the world's biotechnology and pharmaceutical companies, we could realistically hope for a breakthrough in malaria that could give new hopes for billions of people in the developing world. Indeed, once such a breakthrough is made possible, it is hard to imagine that the opportunity will not be grasped. - 1999
The Financial Times
|